
Upper Crossed Syndrome -Pain in the Neck
Upper crossed syndrome (UCS) is becoming incredibly prevalent in our current society. Technology is a particular driving force for this (but not the only cause), which is why terms like “Tech Neck” are starting to come into fashion. Young children through geriatrics are using smaller technology more and more each day, which normally puts us in a forward collapsed posture. By “forward collapsed posture” I refer to a head forward from the body, facing downward, chin tucked, shoulders rounded forward, over-accentuated mid back, stomach out, and a flat low back. Look at anyone using a cell phone, or working at a computer for long hours and you’ll see this very same posture.

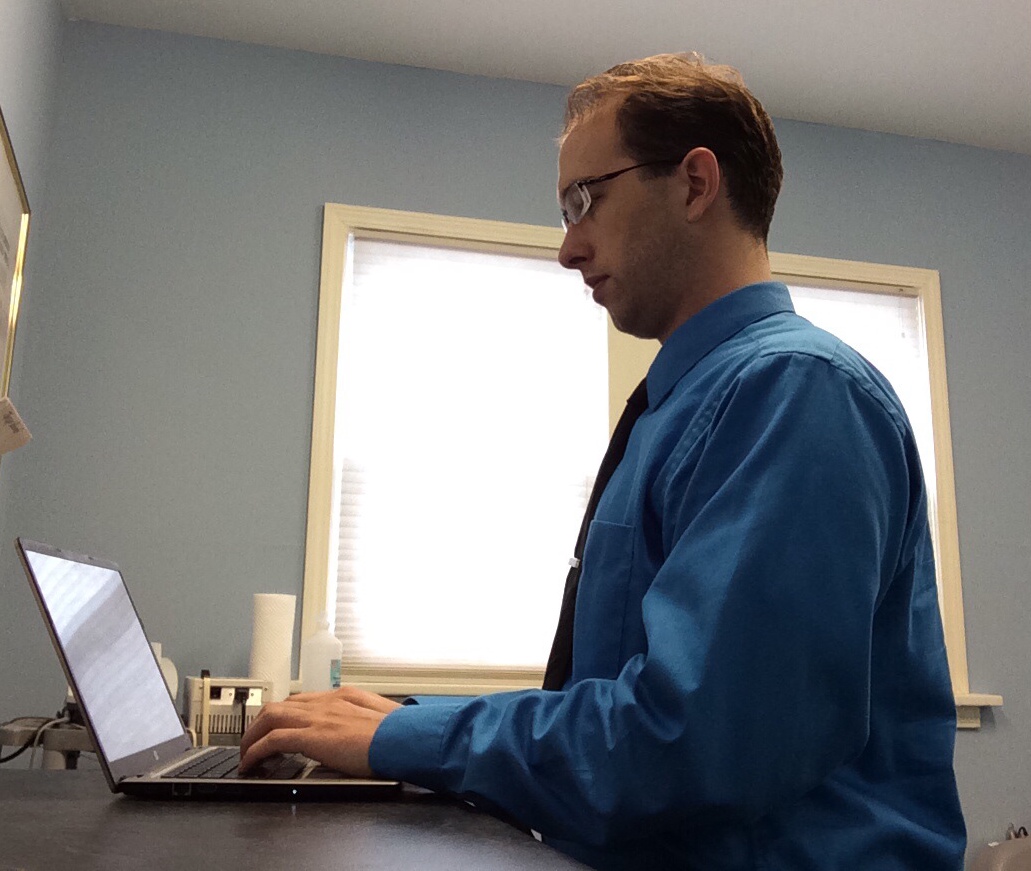
(Dr. Herrington demonstrating upper crossed posture. Note the rounded back and shoulder rolled forward and the head not over the body)
As a Chiropractor, this is awful. As doctors, we look at movement and posture possibly more than anyone, and all of these positions together create a perfect storm of various pain patterns.
(Dr. Herrington demonstrating proper seated posture. Note the straight back and shoulder in line the head/ear. The head is centered over the spine, rather than in front of it)
Upper crossed syndrome was discovered by a physician named Vladimir Janda. In 1979, he published findings of patterning to muscles that fatigued and stressed in very tell tale patterns. These became known as upper crossed, and lower crossed syndromes.
Upper crossed syndrome is classically known for having tight sub occipital muscles, scalenes, upper trapezius, and levator scapulae, while having weak cervical flexors, and rhomboids and lower trapezius. Thus far, this sounds like nothing but some tight muscles and weakness. It’s the pattern that makes all the difference.
What symptoms can Upper Crossed Syndrome (UCS) cause?
UCS can cause pain in the neck, mid back, shoulders, arm, forearm, wrist or hand. Radiating burning pain or numbness, from the neck to the hand, carpal tunnel like pain in the wrist and hand, headaches, migraines, and possible weakness of the hands.
How can Upper Crossed Syndrome (UCS) make all that pain possible?
When the muscles don’t work in the proper way they should, the body must compensate. When it compensates, muscles that wouldn’t normally be used must become engaged to maintain this new (poor) posture. When the head is forward from the body a particular set of muscles called the “scalenes” become very tight and sore. Directly between these 3 muscles on the side of the neck, are the nerves that travel from the spine, through the vertebrae, between the scalene muscles, and down the arm to the hand. If these nerves become inflamed along with the muscles, the pain can be felt all the way into the fingertips. This pain can be very similar to carpal tunnel, without having any of the classic medical symptoms of carpal tunnel syndrome.
As for the headaches and migraines, the trapezius and levator scapulae commonly become over worked and sore, due to constantly being contracted while trying to stretch. This will cause them to inflame, where the muscles cross, and the muscle fibers, along with the slippery connective tissue between them become interwoven. This “knotted” point is commonly called a fascial tigger point. When this point is inflamed, it commonly can pain up the back of the skull and around the ear. This is referred to as the “question mark” headache, as the pain starts in front of the ear, travels around, back down the neck, skips about 1-2” at the base of the neck, and ends at the trigger point at the trapezial/levator cross point.
Migraines have a litany of triggers, many of which are still being researched. Some people get considerable relief when their sub occpital muscles have been relaxed via manual therapy or muscle stretching techniques. The sub occipital muscles share fibers with the posterior atlanto-occipital membrane (a tough membrane that connects the base of the skull to the first cervical vertebra), which itself occasionally has some fiberous connections to the dura mater (the outer membrane around the brain). This connection has been called the myodural bridge. These connections have been noted in some cadaver dissections. No research has been shown to demonstrate the connection between these links, and migraines, but many chiropractic patients report relief after treatment and this is just one possible explanation for such. [1]
Why does this happen?
The large trapezius muscle has two functions, depending on where you reference it. The top half, is meant for lifting and holding the shoulders, in a shoulder shrug “I don’t know” kind of motion. The bottom half is meant from bringing your shoulders backwards and down, as if you are standing up and stretching your arms back. The upper half is very strong, the bottom half isn’t. The upper half is for lifting, the bottom half is for posture.
The cervical flexors, are one of the first muscles groups we acquire use of as a person. When we learn to pick up our large head, as a baby, we are engaging the cervical flexor muscles. They bring the head back, to give, and maintain a nice curve to the cervical spine. This keeps the head centered over the body, and keeps our eyes and ears in optimal positions, in line with the horizon.
The suboccipital muscles are tiny muscles that lay deep under all the large muscle bodies of the neck. They attach the top 2 vertebrae to the skull. They are meant for minor movements of the upper neck and skull, unlike the lower cervical flexor muscles, that are used for much larger motions. If you tip your head up, very slightly to glance at something, you use mostly the sub occpital muscles. If you quickly move your head upwards to look at a bird, you are using your larger cervical flexor muscle groups.
When you sit with a very hunched forward, rolled shoulders you are stretching your lower trapezius and rhomboids. The pectoralis major, (the big, front chest muscle) is much larger and stronger than the lower trapezius/rhomboid pair (smaller, weaker, mid back postural muscles) so in this chronically contracted state, the weaker two muscles are very easily damaged. Trying to fight against this much stronger muscle, is like one person trying to win a tug of war contest against a car.
Sitting in this posture, the shoulders are raised, holding the upper trapezius and levator scapulae in a contracted state, which inflames and damages the muscle over time. These two muscles are for lifting the scapula (shoulder blade) in short heavy lifting bursts. Not for maintained posture. With these two muscles engaged, the cervical flexor muscles are naturally inhibited. This inhibition causes the subocciptal muscles to become the main movers of the skull, given that small digital screens do not require vast neck movements to look at for hours at a time. The longer the head is held forward from the body, the longer the scalene muscles are strained while trying to hold the head in that position. Holding a weight away from the body, is much harder than holding it close to the body. The cervical flexor muscles, which are still inhibited from the poor shoulder posture, cannot hold the head in its proper position. This causes significant damage and inflammation to the scalenes over time, which further aggravates the nerves in the shoulder and arms.
What can be done to alleviate Upper Crossed Syndrome (UCS)?
This is why it is very important to consider the whole body, rather than just the place a person experiences pain. A pain in the hand might originate from the neck, or the abdomen. (Moving your shoulders/chest while breathing, instead of diaphragmatic breathing can over tax the shoulder and chest muscles, which in turn will tax the neck musculature, which will contribute to upper crossed syndrome, which can cause carpal tunnel like symptoms). A proper diagnosis of the source of the problem, followed by conservative treatment, and proper rehabilitation typically resolves these cases very effectively. The best part about this syndrome is the fact that with diligence on the behalf of the patient, complete resolution of symptoms is typically expected in time.
[1] Enix, D. The obliquus capitis inferior myodural bridge. Clinical Anatomy, 450-454.